
Treatment Strategy for Pyoderma Gangrenosum: Skin Grafting with Immunosuppressive Drugs
 , ,
, ,
Abstract
:1. Introduction
2. Case Reports
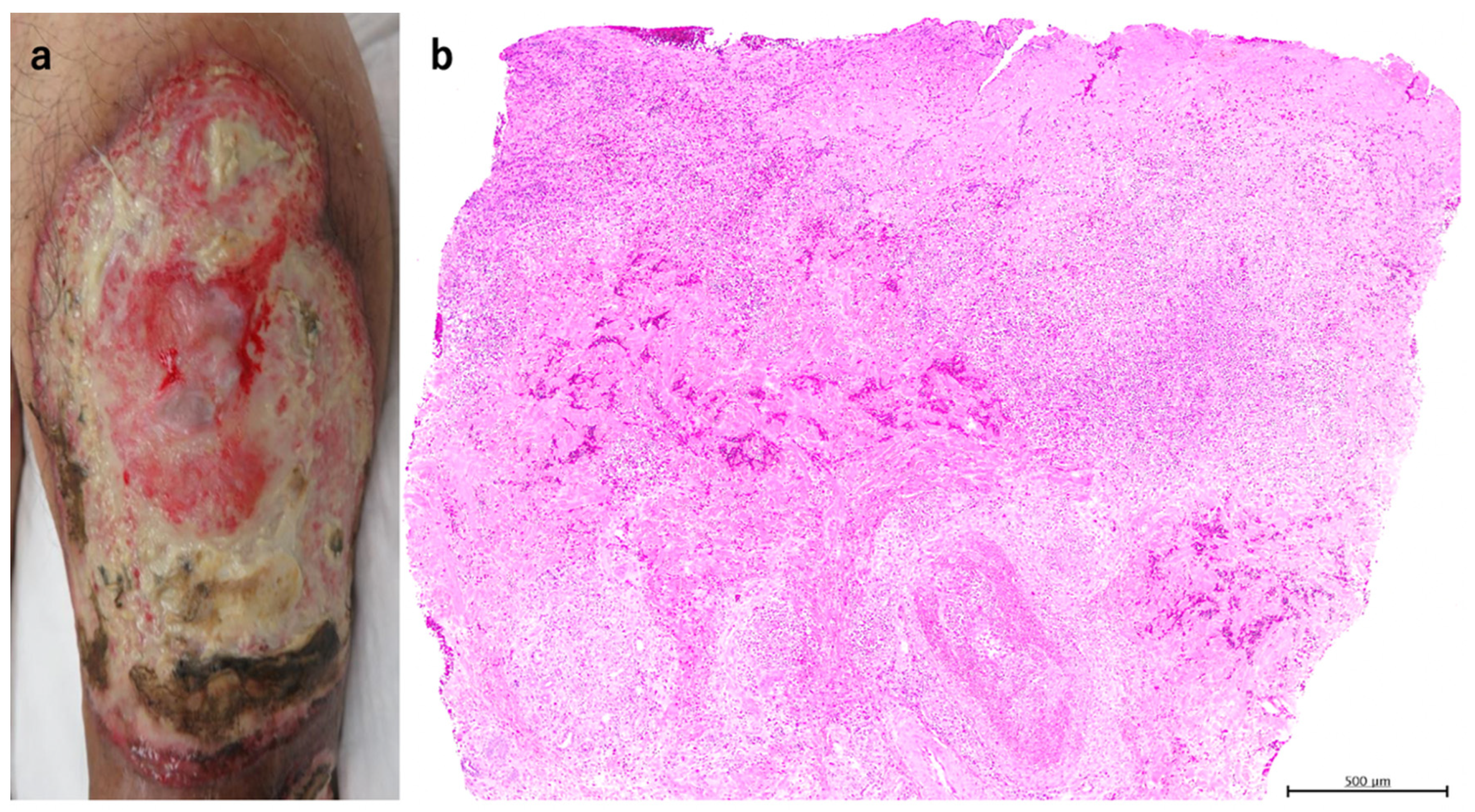
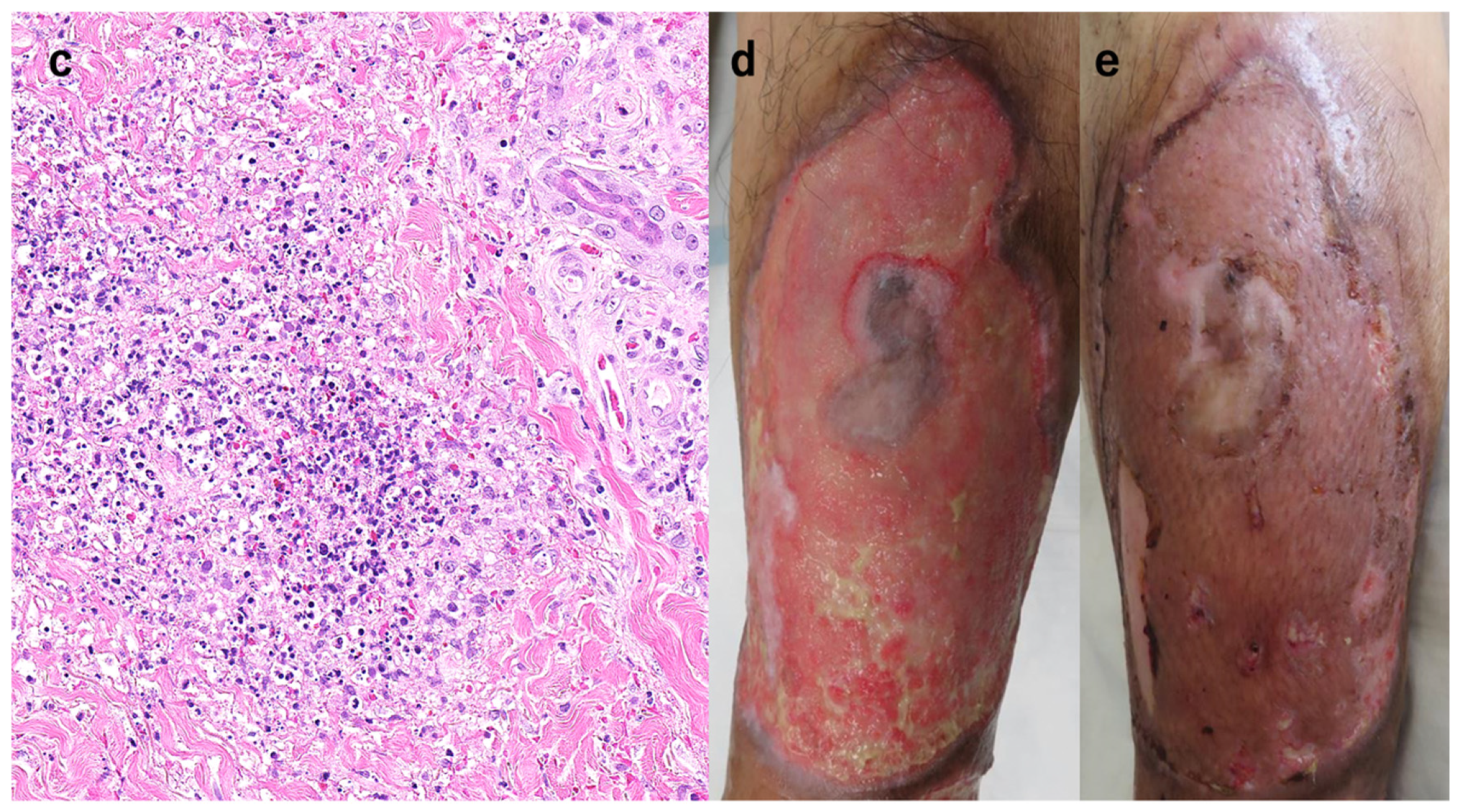
2.1. Case 1
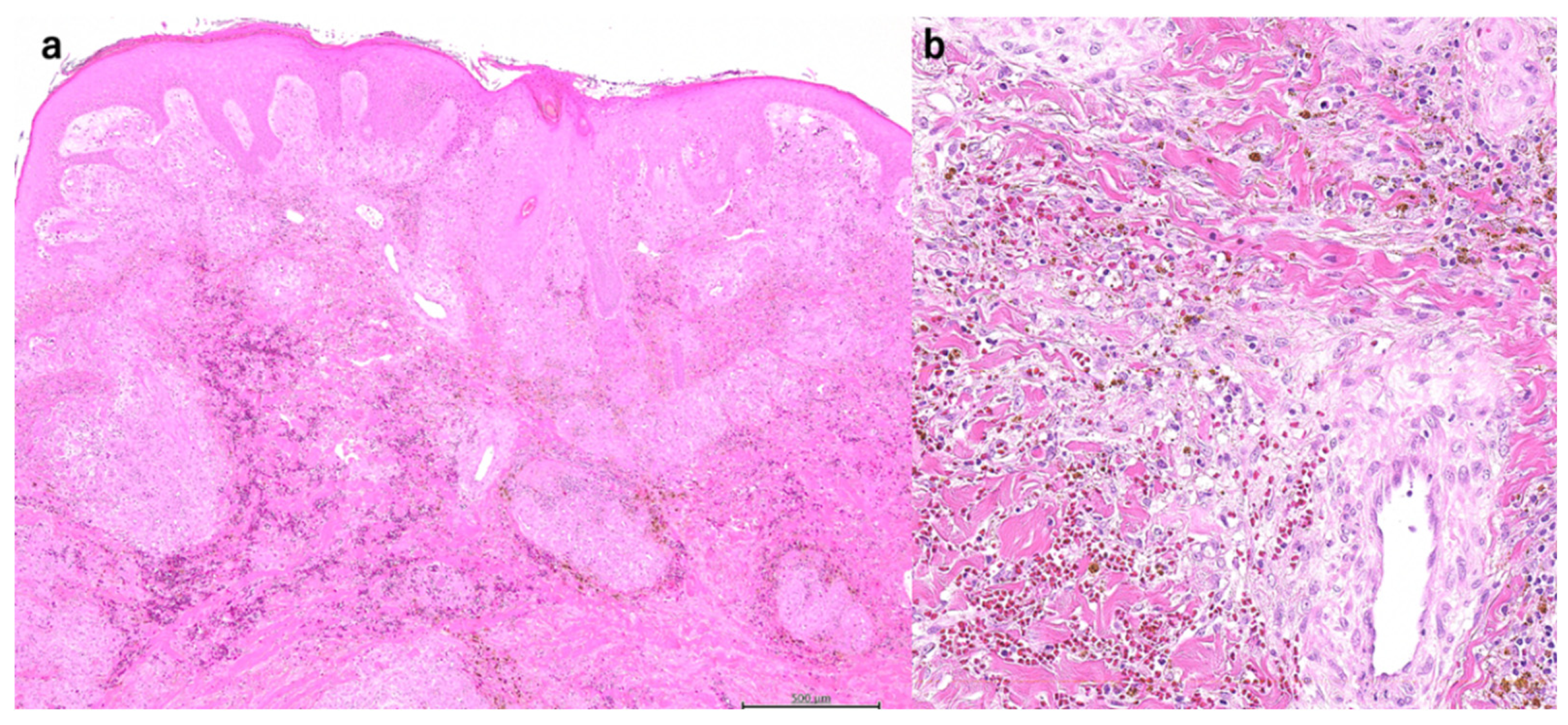
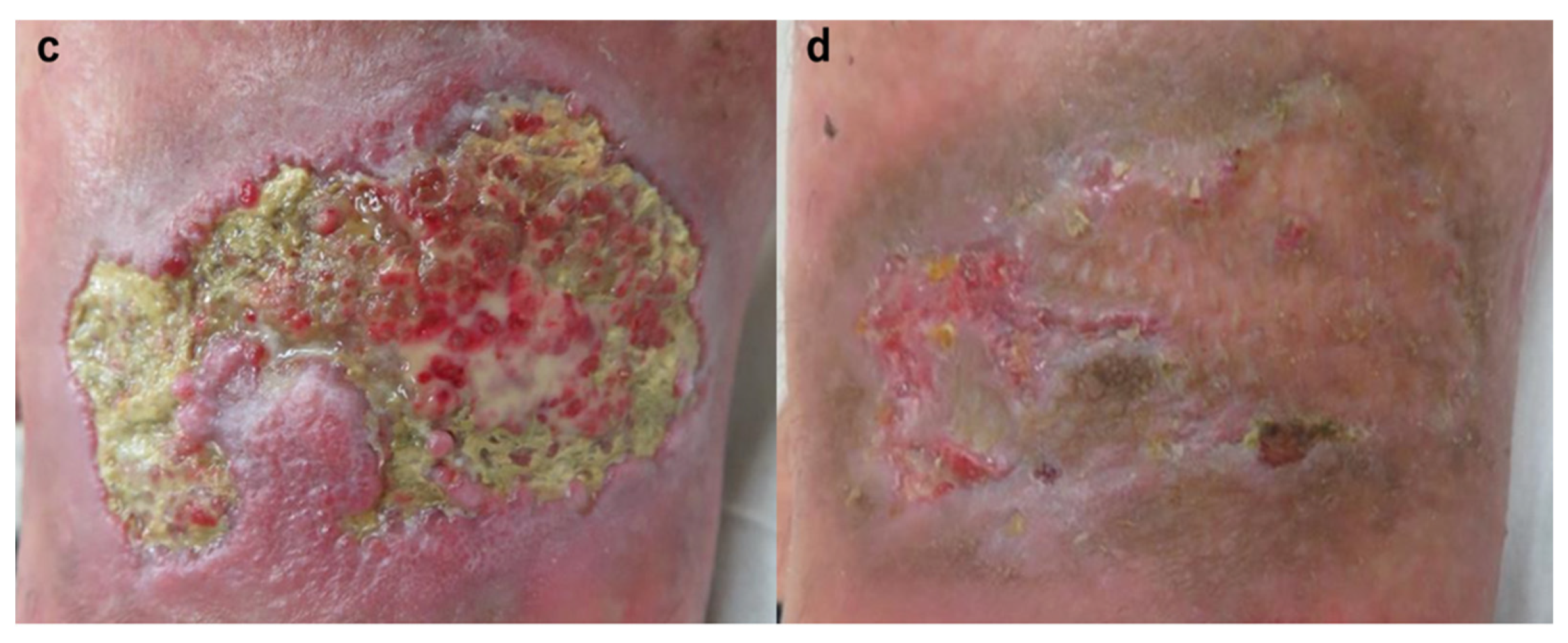
2.2. Case 2
2.3. Case 3
2.4. Case 4
3. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Maverakis, E.; Marzano, A.V.; Le, S.T.; Callen, J.P.; Bruggen, M.C.; Guenova, E. Pyoderma gangrenosum. Nat. Rev. Dis. Primers 2020, 6, 81. [Google Scholar] [CrossRef] [PubMed]
- Ruocco, E.; Sangiuliano, S.; Gravina, A.G.; Miranda, A.; Nicoletti, G. Pyoderma gangrenosum: An updated review. J. Eur. Acad. Dermatol. Venereol. 2009, 23, 1008–1017. [Google Scholar] [CrossRef] [PubMed]
- Marzano, A.V.; Borghi, A.; Meroni, P.L.; Cugno, M. Pyoderma gangrenosum and its syndromic forms: Evidence for a link with autoinflammation. Br. J. Dermatol. 2016, 175, 882–891. [Google Scholar] [CrossRef] [PubMed]
- Bennett, M.L.; Jackson, J.M.; Jorizzo, J.L.; Fleischer, A.B., Jr.; White, W.L.; Callen, J.P. Pyoderma gangrenosum. A comparison of typical and atypical forms with an emphasis on time to remission. Case review of 86 patients from 2 institutions. Medicine 2000, 79, 37–46. [Google Scholar] [CrossRef] [PubMed]
- Turner, R.B.; Emer, J.J.; Weill, M.; Winterfield, L.; Friedman, S.; Qureshi, A.A. Rapid resolution of pyoderma gangrenosum after treatment with intravenous cyclosporine. J. Am. Acad. Dermatol. 2010, 63, e72–e74. [Google Scholar] [CrossRef] [PubMed]
- Kontochristopoulos, G.J.; Stavropoulos, P.G.; Gregoriou, S.; Zakopoulou, N. Treatment of Pyoderma gangrenosum with low-dose colchicine. Dermatology 2004, 209, 233–236. [Google Scholar] [CrossRef] [PubMed]
- Hinterberger, L.; Muller, C.S.; Vogt, T.; Pfohler, C. Adalimumab: A treatment option for pyoderma gangrenosum after failure of systemic standard therapies. Dermatol. Ther. 2012, 2, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marasca, C.; Fontanella, G.; Annunziata, M.C.; Marasca, D.; Fabbrocini, G. Adalimumab plus topical tacrolimus for the treatment of pyoderma gangrenosum: Report of a case. Int. Wound J. 2019, 16, 1047–1048. [Google Scholar] [CrossRef] [PubMed]
- Yamasaki, K.; Yamanaka, K.; Zhao, Y.; Iwano, S.; Takei, K.; Suzuki, K.; Yamamoto, T. Adalimumab in Japanese patients with active ulcers of pyoderma gangrenosum: Twenty-six-week phase 3 open-label study. J. Dermatol. 2020, 47, 1383–1390. [Google Scholar] [CrossRef] [PubMed]
- Yamasaki, K.; Yamanaka, K.; Zhao, Y.; Iwano, S.; Takei, K.; Suzuki, K.; Yamamoto, T. Adalimumab in Japanese patients with active ulcers of pyoderma gangrenosum: Final analysis of a 52-week phase 3 open-label study. J. Dermatol. 2022, 49, 479–487. [Google Scholar] [CrossRef] [PubMed]
- Almeida, I.R.; Coltro, P.S.; Goncalves, H.O.C.; Westin, A.T.; Almeida, J.B.; Lima, R.; Silva, M.F.; Farina Junior, J.A. The role of negative pressure wound therapy (NPWT) on the treatment of pyoderma gangrenosum: A systematic review and personal experience. Wound Repair Regen. 2021, 29, 486–494. [Google Scholar] [CrossRef] [PubMed]
- Nakayama, Y.; Akeda, T.; Iida, S.; Habe, K.; Yokota, N.; Matsushima, Y.; Nakai, Y.; Kondo, M.; Yamanaka, K. Whether to maintain or strengthen the treatment for pyoderma gangrenosum ulcerative type may depend on the response after two to four-week treatment intervention: The outcome of three cases with details clinical course. Clin. Case Rep. 2021, 9, e04690. [Google Scholar] [CrossRef] [PubMed]
- Goto, H.; Okada, Y.; Watanabe, S.; Danno, K.; Yamamoto, S.; Ishiura, R.; Nakayama, Y.; Mitsui, K.; Ueki, A.; Nakai, Y.; et al. Successful Treatment of Ulcerative-Type Pyoderma Gangrenosum with a Combination Therapy of Oral Prednisolone, Vacuum-Assisted Closure, and Skin Grafting. Case Rep. Dermatol. 2021, 13, 497–501. [Google Scholar] [CrossRef] [PubMed]
- Ergun, T. Pathergy Phenomenon. Front. Med. 2021, 8, 639404. [Google Scholar] [CrossRef] [PubMed]
- Eisendle, K.; Thuile, T.; Deluca, J.; Pichler, M. Surgical Treatment of Pyoderma Gangrenosum with Negative Pressure Wound Therapy and Skin Grafting, Including Xenografts: Personal Experience and Comprehensive Review on 161 Cases. Adv. Wound Care 2020, 9, 405–425. [Google Scholar] [CrossRef] [PubMed]
- Kodumudi, V.; Lam, D.; Rajput, K. Pain Control in Dermatologic Conditions. Curr. Pain Headache Rep. 2021, 25, 38. [Google Scholar] [CrossRef] [PubMed]
- Kaddoura, I.L.; Amm, C. A rationale for adjuvant surgical intervention in pyoderma gangrenosum. Ann. Plast. Surg. 2001, 46, 23–28. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case 1 | Case 2 | Case 3 | Case 4 | |
|---|---|---|---|---|
| Disease duration until initiation of immunosuppressive treatment | 34 months | 1 month | Over 10 years * | 2 years * |
| Time from start immunosuppressive treatment to surgery | 2 months | 13 months | 2 months * | 2 weeks * |
| Immunosuppressant dose during surgery | Prednisolone 10 mg | Prednisolone 5 mg + adalimumab | Prednisolone 12 mg + Tacrolimus 6 mg | Prednisolone 20 mg |
| CRP at the time of surgery | 0.48 mg/dL | 0.24 mg/dL | 0.44 mg/dL | 0.02 mg/dL |
| Time from onset to surgery | 3 years | 14 months | Over 10 years | 2 years |
| Other autoimmune diseases | None | None | Existence | Existence |
| Transplantation site | Ventral lower leg | Lateral lower leg | Medial lower leg | Medial to dorsal lower leg |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nishimura, M.; Mizutani, K.; Yokota, N.; Goto, H.; Akeda, T.; Kitagawa, H.; Habe, K.; Hayashi, A.; Yamanaka, K. Treatment Strategy for Pyoderma Gangrenosum: Skin Grafting with Immunosuppressive Drugs. J. Clin. Med. 2022, 11, 6924. https://doi.org/10.3390/jcm11236924
Nishimura M, Mizutani K, Yokota N, Goto H, Akeda T, Kitagawa H, Habe K, Hayashi A, Yamanaka K. Treatment Strategy for Pyoderma Gangrenosum: Skin Grafting with Immunosuppressive Drugs. Journal of Clinical Medicine. 2022; 11(23):6924. https://doi.org/10.3390/jcm11236924
Chicago/Turabian StyleNishimura, Mai, Kento Mizutani, Naho Yokota, Hiroyuki Goto, Tomoko Akeda, Hiroshi Kitagawa, Koji Habe, Akinobu Hayashi, and Keiichi Yamanaka. 2022. "Treatment Strategy for Pyoderma Gangrenosum: Skin Grafting with Immunosuppressive Drugs" Journal of Clinical Medicine 11, no. 23: 6924. https://doi.org/10.3390/jcm11236924